
Be Proactive About Your Brain Health
The Alzheimer’s Plasma Extension (APEX) Study is an observational study on Alzheimer’s disease (AD) related brain changes. An observational study is where researchers look at (or observe) changes over time without any study treatments.
In this study, researchers hope to learn about the factors that may preserve memory and thinking in older individuals who do not develop elevated amyloid levels in the brain.
What is amyloid and how does it relate to Alzheimer’s disease?
Amyloid is a protein fragment that the body produces normally. With aging, and especially in AD, amyloid begins to accumulate in the brain forming amyloid plaques. Amyloid has been associated with an increased risk of memory loss and cognitive decline.
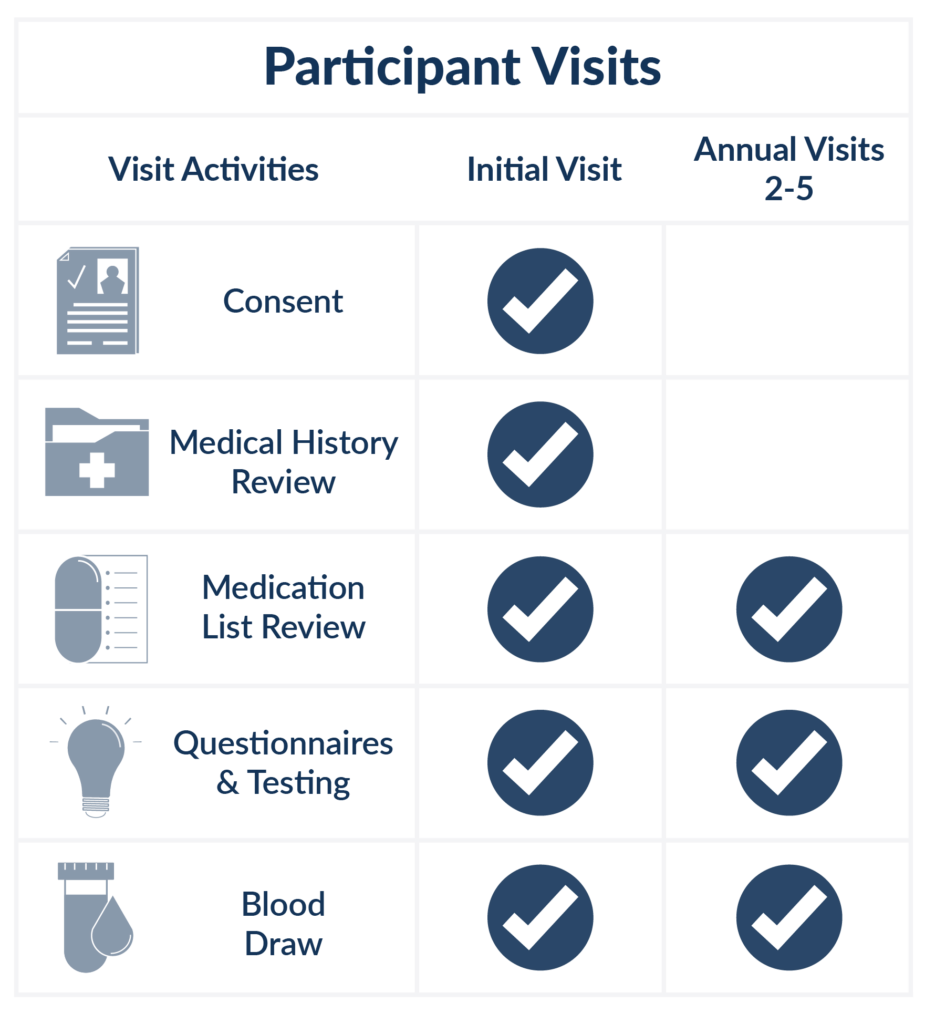
What is involved?
- One in-person visit every year for four years
- Blood samples, memory tests and questionnaires will be collected
What is the value of participating in the APEX Study?
The APEX Study is an opportunity to be proactive about your brain health and help researchers make progress in finding future potential treatment for AD and other causes of dementia. Researchers will carefully monitor your brain health and it is an opportunity to ask questions related to your brain health. You may also learn of other research opportunities that you may be suitable for.

What to know about participating in the APEX Study?
- Participants may be reimbursed for their time
- Participant transportation may be provided for study-related visits
- Study participation and procedures at no cost to you
- No study partner needed
- Minimal yearly time commitment
- Participant diversity, inclusion, and representation are vital
- Data privacy is a top priority

Commitment to Inclusion and Representation
The APEX Study seeks individuals from all races, ethnicities, genders, sexual orientations, economic backgrounds, and geographies to increase our understanding of AD.
Be proactive about your brain health. Join the APEX Study and help inform future clinical trials for Alzheimer’s disease. If you are interested in participating in the APEX Study or if you have any additional questions, please reach out to your local study staff team.